Aor Insurance Form
Fillable Online Aor Form 071406 Carlton Wright Insurance Fax Email Print Pdffiller
Fillable Online Appointment Of Representative Aor Form Pdf Health Net Fax Email Print Pdffiller
Https Www Citizensfla Com Documents 20702 41806 Aor Commercial Form B433025f 19cf 45b9 B2c2 E56d6f198953 Version 1 0
Https Www Uhcprovider Com Content Dam Provider Docs Public Claims Uhccp Aor Form Pdf
Fillable Online Agent Of Record Aor Form Bmylahcorgb Fax Email Print Pdffiller
Http Www Sgatn Com Uploads 1 3 1 9 13197303 Bor Pdf
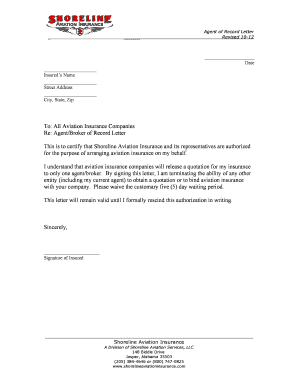
Sample aor letter from insured date insurance company name address re.
Aor insurance form. Producer code date insured s signature date title if applicable company name if applicable fax a c no. Applicant name business name street address city state postal zip code. Utilizing the back offices of a larger brokerage firm allows aor insurance the ability to broker national accounts and scale down our services for smaller clients. Skadsberg randy w subject.
Home aor insurance application form. Unitedhealthcare community plan authorization of review aor form claim appeal author. Phone a c no ext. Please be advised that effective date we have appointed the xyz agency as our agent of record with regard to insurance and bonding requirements.
Member authorization form for a designated representative to appeal a determination. Previously completed for any other insurance representative for the this authorization replaces any other authorization that may have been insured s signature date. For use with claim appeal process when unable to access online tools. Date mm dd yyyy insurance company name code.
Phone email website date established limit of insurance 500 000 00 1 000 000 00 2 000 000 00 other. Insurance company name city of insured state of insured zip code of insured street address of insured title if applicable company name if applicable stated lines of business.
Https Www11 Anthem Com Agent Va F5 S2 T0 Pw B156919 Pdf Refer Ahpagent

Humana Aor Form Fill Online Printable Fillable Blank Pdffiller
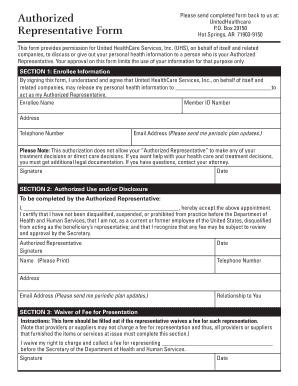
United Healthcare Designation Of Authorized Representative Form Fill Online Printable Fillable Blank Pdffiller Pdffiller
Https Medicareplansstcharles Com Wp Content Uploads 2017 07 Anthem Aor Pdf

Nj St7 Fill Online Printable Fillable Blank Pdffiller Pdffiller
Fillable Online Agent Of Record Letter Aor Shoreline Aviation Insurance Fax Email Print Pdffiller

Fillable Online Agent Of Record Aor Transfer Form Please Complete The Fax Email Print Pdffiller

Rescinding Bor Template Fill Online Printable Fillable Blank Pdffiller
Guide To Reporting Loss Of Health Care Coverage Online Assister Central Mnsure

Fillable Online Claim Form Healthcare Insurance Aon Student Insurance Fax Email Print Pdffiller
Https Cdn1 Brighthealthplan Com Docs Ma Resources 2019 Appeal Form Az Multi Ma Pdf

Image Result For Insurance Form Design Diagramacao