Election To Keep Medical Insurance Form

Power Of Attorney Template For Children Impressive Free Montana Minor Child Power Of Attorney Form Pdf Of 32 Power Of Attorney Power Of Attorney Form Attorneys

Standards Of Operations Employee Handbook Spa And Salon Etsy In 2020 Employee Handbook Evaluation Employee Business Template

1099 Misc Software To Create Print And E File Form 1099 Misc Fillable Forms Irs Forms Tax Forms

Healthcare Forms Form Templates Jotform

Form 1095 C Employer Provided Health Insurance Offer And Coverage
Https Www Bluecrossmn Com Sites Default Files Dam 2020 06 P11ga 13557156 F8026r07 Cobra 20continuation 20election 20notice Fillable Enabled Pdf
Medical insurance records medical questionnaires benefit enrollment forms and benefit claims doctors notes accommodation requests and leave of absence records.
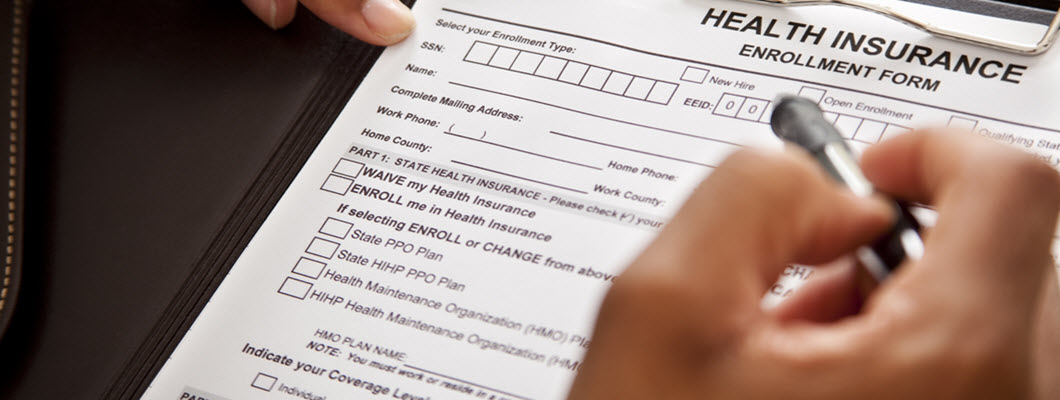
Election to keep medical insurance form. Or elect not to enroll in the fehb program employees only or change your fehb enrollment. 888 531 5781 fax to. The notice will state the date your coverage will end and provide you with the opportunity to. Health care id cards will be mailed to your home within 2 3 weeks after your enrollments are processed.
Uses for standard form sf 2809 use this form to. Health insurance coverage for individuals families and small businesses. Employer for insurance premium fmla leave employee name company revised 3 17 10 1110 n. Medi cal providers and billers may view and download the following forms.
Suite b kennewick wa 99336 phone. 509 735 7668 i understand that the family and medical leave act fmla allows me to continue as a participant in the pay plus benefits group. Program provider election form and agreement dhcs 7012 hospital. Department of health and human services through the centers for medicare medicaid services cms has jurisdiction with respect to the cobra continuation coverage requirements of the phs act that apply to state and local government employers including counties municipalities and public school districts and the group health plans.
509 735 1143 toll free. If you fail to return the benefits continuation election form to the leaves office prior to the beginning of your leave your insurance is subject to cancellation. Switch designated eligible family member. Or enroll or reenroll in the fehb program.
If coverage is cancelled you will need to. Report all discrepancies immediately to the office of human resources employee service center at 855 278 5081 orhresc asu edu. Or cancel your fehb enrollment. Health benefits election form form approved.
Health benefits election form generally you will make elections to enroll not to enroll to change enrollment or to cancel enrollment on the health benefits election form sf 2809. The form cms l457 is a notice from the centers for medicare medicaid services that your medical part b medical insurance will end per your request the form cms l457 is a notice from the centers for medicare medicaid services that your medical part b medical insurance will end per your request. The sf 2809 may be in either paper or electronic format.

Free Sample Business Trust Agreement Form Template Real Estate Forms Word Template Real Estate Templates
Https Www Vantagehealthplan Com Documents Businessowners Cobra Notice And Electionform Pdf

Nih Format Cv Template Kairo 9terrains Co In Nih Biosketch New Format Template 54303 Study Notes Writing A Bio Printing Labels

Vermonters Spend 12th Highest In Nation On Healthcare Vermont Business Magazine Healthcare Costs Health Care Health Insurance Plans

Pin On Free Legal Liability Waiver Forms

90 Day Employee Evaluation Form Best Of Free 14 90 Day Review Forms In Pdf In 2020 Employee Evaluation Form Evaluation Form Employment Reference Letter

Should Student Journalists Carry Press Passes Student Press Student Pressing

Before Releasing The Redacted Mueller Report Attorney General William Barr Claimed At A Press Conference That Its Findings Were Fa Barr Read Letters Lettering

Found On Google From Pinterest Com Job Application Form Job Application Template Employment Application

Read Mueller S Letter To Ag Barr Criticizing His Framing Of The Russia Report S Findings
How To Make Changes To Your Health Plan
Https Www Tdi Texas Gov Rules 2013 Documents Titleruleexhibi Pdf

Is This Trump Army Fundraising Email Real In 2020 Fundraising Email Fundraising Trump
