Healthplex Insurance Form
Fillable Online Nyc Healthplex Dental Claim Form Nyc Gov Nyc Fax Email Print Pdffiller
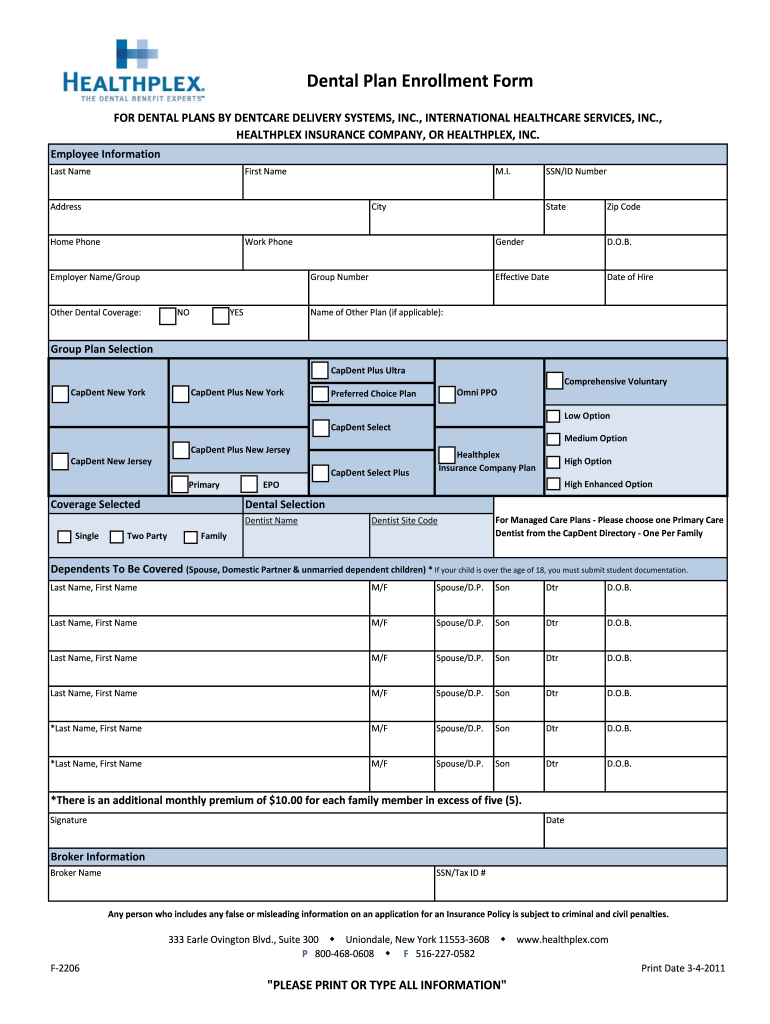
Enrollment Healthplex Dental Fill Out And Sign Printable Pdf Template Signnow
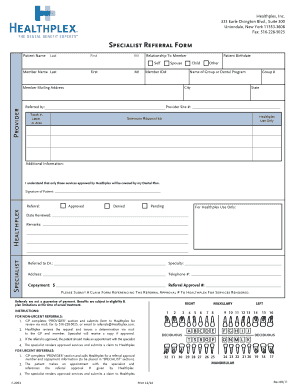
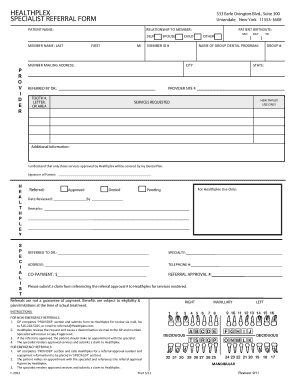
Healthplex Referral Form Fill Online Printable Fillable Blank Pdffiller
Https Www Healthplex Com Doc No F 2203
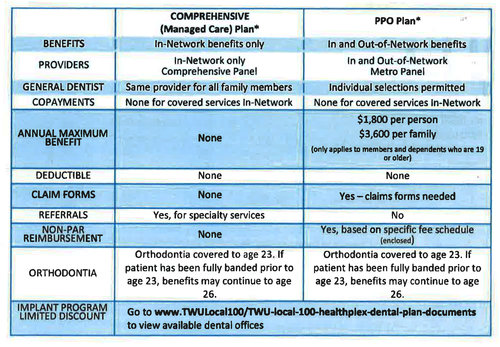
Twu Local 100 Healthplex Dental Plan Documents Twu Local 100
Healthplex Fill Online Printable Fillable Blank Pdffiller
Employer name group name 10.
Healthplex insurance form. Patient s relationship to person named in 5 11. 516 542 2614 all information must be printed attention. Healthplex provider manual. The form is designed so that the name and address item 3 of the third party payer receiving the claim insurance company dental benefit plan is visible in a standard 9 window envelope window to the left.
You may setup a recurring payment or make a one time payment. Employer name group name 10. Please complete part b of the reverse side of this form examining doctor or optometrist information and sign your name. Healthplex offers access healthplex dental discount plan alternative to dental insurance.
Po box 211672 eagan mn 55121 see reverse side for additional information 9. Ada claim form. Provider inquiry request for clarification form. Other insurance company dental bene t plan name address city state zip code.
Ada claim form. F 2649 dental care infographic web flyer. Please be sure you have provided the employee s social security. Braces removal and retainer consent form.
Message from healthplex participating provider networks have always been a key component of healthplex s dental programs. Healthplex has dental insurance and dental discount plans for individuals and groups of all sizes. Send the completed benefit request form directly to the healthplex office. We recognize the value of a strong relationship with the dental community and have always attempted to balance the needs of our dentists with the needs of our enrollees.
Po box 9255 uniondale ny 11553 9255 9. It includes orthodontics with access to more than 95 000 dental access points. Send completed forms to. We also have a dental discount implant program for our existing dental insurance customers.
Dental preferred provider nomination request form. Credentialing package dentist personal profile. Healthplex is one of the largest dental insurance providers in the state of ny. Healthplex provider web portal guide.
Send completed forms to. Please fold the form using the tick marks printed. W 9 office information form. Our dental discount plans is offered in and all other states.
A separate form should be submitted for each family member. Healthplex clinical criteria master 2019 essential.
Https Www Healthplex Com Doc Fn Youngsmiles Payments
Https Www Healthplex Com Doc Fn Youngsmiles Policy
Https Www Healthplex Com Provider Doc Fn Ppofacts Gg 293r2
Https Www Healthplex Com Provider Doc Fn Ppofacts Gg1010a 8a
Https Www Healthplex Com Pdfs Benefits Schedule Of Benefits Aso Pdf
Https Www Healthplex Com Doc Fn Hic Adult Shop Cert

Csea Local 880 Healthplex Dental Claim Form Back Facebook
Https Www Healthplex Com Provider Doc Fn Ppofacts Gg 453
Https Www Healthplex Com Doc Fn Hic Ped Shop Cert