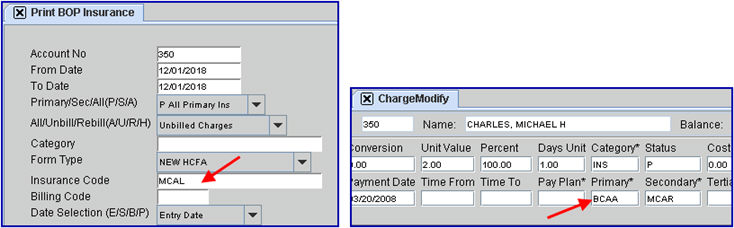
Mcal Change Of Insurance Form

Pin On Love S Helping Hands
Http Www Dhcs Ca Gov Formsandpubs Forms Forms Mc355 Pdf
Other Coverage
Https Www Dhcs Ca Gov Formsandpubs Forms Forms Mc210a Pdf
Medi Cal Id Card L A Care Health Plan
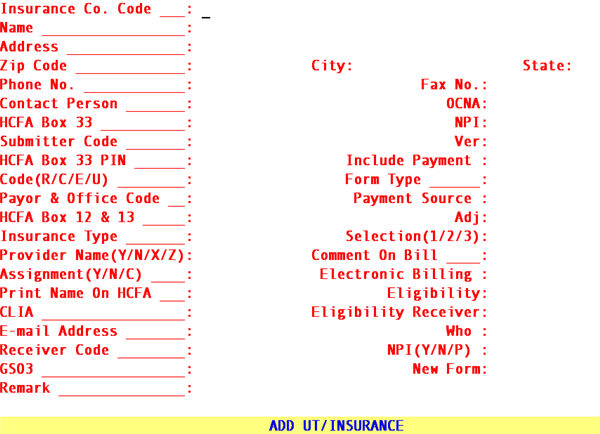
Utility Insurance
Quality assurance fee program.
Mcal change of insurance form. Health insurance premium program hipp application. Fill out the patient request for medical payment form cms 1490s you ll find the address for form submission in the instructions. If you need any assistance please call us at 1 800 638 5000. Back to forms by program.
We ll try to make the process of filing a life insurance claim as simple as possible. If the beneficiary is a trust or entity use this form. If waiving dental coverage a waiting period may apply if coverage is requested at a later date. 2 12 employee must sign this form for anything other than a termination of employment.
For each beneficiary please complete and return one of the forms below. Employee information as it appears on id card first name last name. Mba insurance application and or change form required employee name first mi last name prior name if changing. Of insurability and that insuring carrier will have the right to refuse my request for insurance.
Change form medical coverage is a product of physicians health plan dental insurance is a product of delta dental plan of michigan. For information about completing and submitting these forms please review the appropriate provider manual section. Third party liability notification. Please sign the bottom of this form.
Medi cal providers and billers may view and download the following forms. You can also get this form in spanish. If the beneficiary is an individual use this form. Health insurance premium payment program.
Dental request for access to protected health information.
Https Files Medi Cal Ca Gov Pubsdoco Outreach Education Workbooks Modules Bb Ub04 Bb Pdf
Http Files Medi Cal Ca Gov Pubsdoco Outreach Education Workbooks Modules Bb Soc Bb Pdf
Https Www Greenwichct Gov Agendacenter Viewfile Archivedagenda 12162019 1373 Packet True
Https Www Leegov Com Files Bocc Old 20agendas 2007 04 10 07 Consent C9b Pdf
Hcfa Printing Troubleshooting
Https Www Dhcs Ca Gov Formsandpubs Forms Forms Mced Mc Forms Mc219 Eng 1115 Pdf
Encounter Generic
Https Www Town Canton Ma Us Documentcenter Home View 1705

Confluence Mobile Wiki Ucsf
Https Www Utopiafiber Com Wp Content Uploads 2019 10 Uia Series 2019 2550000 Morgan City Project Telecommunications Electric Utility And Sales Tax Revenue Bonds Official Statement Pdf
Https Pdfs Semanticscholar Org Ab2c 4d9d9d353aab5391a0e58eddc4df577bfd5e Pdf
Http Www Dhcs Ca Gov Formsandpubs Forms Forms Mc 20information 20notices Mc007eng 0414 Pdf
