Metlife Designate Primary And Secondary Insurance Form
Metlife Beneficiary Form Fill Out And Sign Printable Pdf Template Signnow
Fillable Online Metlife Beneficiary Designation Form Jy6004 Fax Email Print Pdffiller
Met Life Life Insurance Beneficiary Form Pdf
Https Das Nebraska Gov Materiel Purchasing 5956 Responses 5956 20z1 20metlife 20proposal 20response 20to 20post Pdf
Https Investor Brighthousefinancial Com Static Files 72cea16f Ffb4 4e1c Bde3 9853d7e449f7
Https Www Metlife Com Content Dam Metlifecom Us Homepage Countyofsandiego Pdf Cosd Life Plan Summary 2018 Pdf

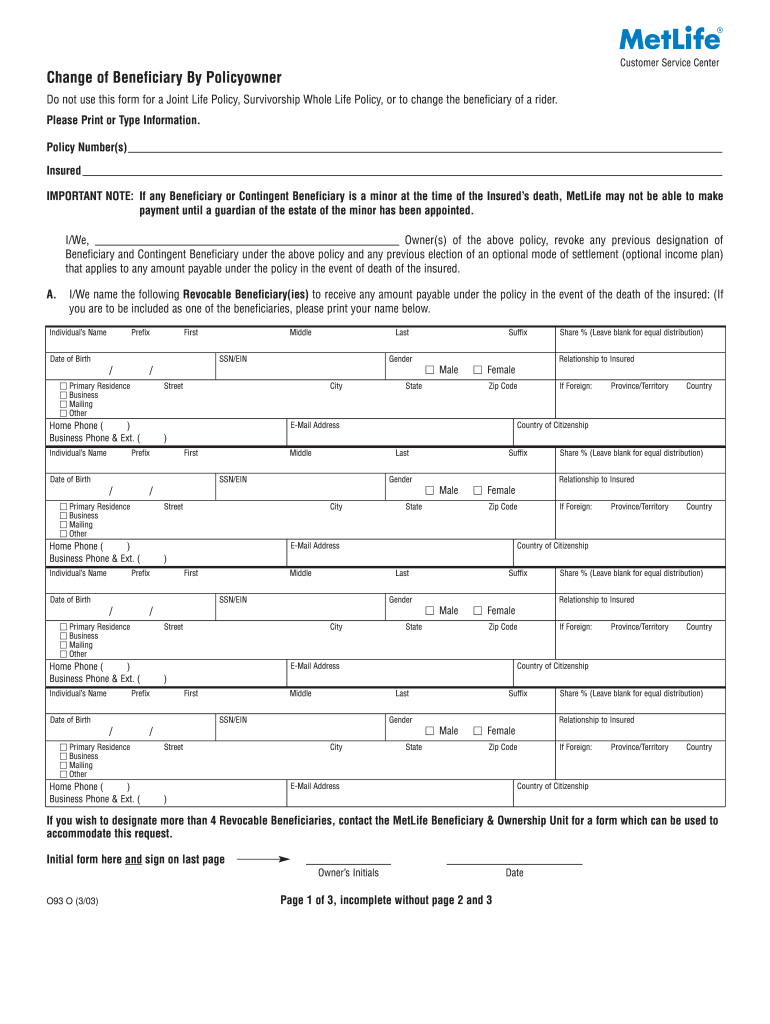
Gather the name s date s of birth social security tax id number s and contact information for all of your beneficiaries.
Metlife designate primary and secondary insurance form. Phishing is a fraudulent attempt to obtain an individual s personal information often through a misleading email text or other online communication. For each beneficiary please complete and return one of the forms below. If you need any assistance please call us at 1 800 638 5000. Phishing is a fraudulent attempt to obtain an individual s personal information often through a misleading email text or other online communication.
Metlife has become aware of a recent phishing attack against some of our customers. Please contact metlife or your plan administrator for complete details. Insurance coverage insured by metlife. Disability insurance is issued by metropolitan life insurance company on idi2000 p nc idi2000 p nc ml idi2000 p gr ah 5 88 ah 6 90 ah 7 96 ca ah 8 96 ca and idip12 01 idip12 05 idip12 08.
Metlife disability claims po box 14590 lexington ky 40511 4590 fax. If the beneficiary is a trust or entity use this form. Provide the requested information including the beneficiary type primary or contingent and the proceeds for each. Designation form for each account.
At the bottom of the form fill in the name of the insured person or owner if assigned the daytime phone number address and sign and date the form. If there is more than one owner all owners must sign. To name additional beneficiaries attach a separate page. Fill in the primary beneficiary ies and contingent beneficiary ies if any.
We ll try to make the process of filing a life insurance claim as simple as possible. Please make a copy of the completed form for your records. Keeping your personal information secure is a top priority of metlife. If the beneficiary is an individual use this form.
Mail above form to. Keeping your personal information secure is a top priority of metlife. The secondary health insurance plan unlike the primary health insurance plan under the coordination of benefits can take into consideration what health insurance benefits were provided to the patient in the primary health insurance plan. This form must reflect all beneficiaries both primary and contingent who should receive the proceeds of the policy ies listed below.
Electronic funds transfer eft authorization form complete sign and mail fax this form to metlife to authorize electronic funds transfers of your disability insurance payments directly to your bank. This form applies to all metlife companies. For each primary and contingent beneficiary listed enter the. Metropolitan life insurance company attn.
Sign and date these page s making sure the date is the same as the date next to the signature on this form.
Pierce Group Benefits
Certificate Of Insurance Schreiner University
Https Eforms Metlife Com Wcm8 Pdffiles 28888 Pdf
Https Www Baylor Edu Hr Doc Php 234603 Pdf
A Guide To Life Insurance New Business Forms Pdf Free Download
Https Www Wabtec Com Uploads Outlinedrawings 2018 Metlife Standard Dental Booklet Pdf
Https Cache Hacontent Com Ybr R515 02274 Ybr Ybrfndt Downloads Sipsummplandescpdf Pdf
Http Www Asante Org App Files Public 2287 139828 Asante Cert17 Gcert2000 Dent Core 01 01 15 Pdf
Https Oda Org Assets Resources Diwg Meeting Materials June 2013 Pdf

Contract Records Change Form Metlife

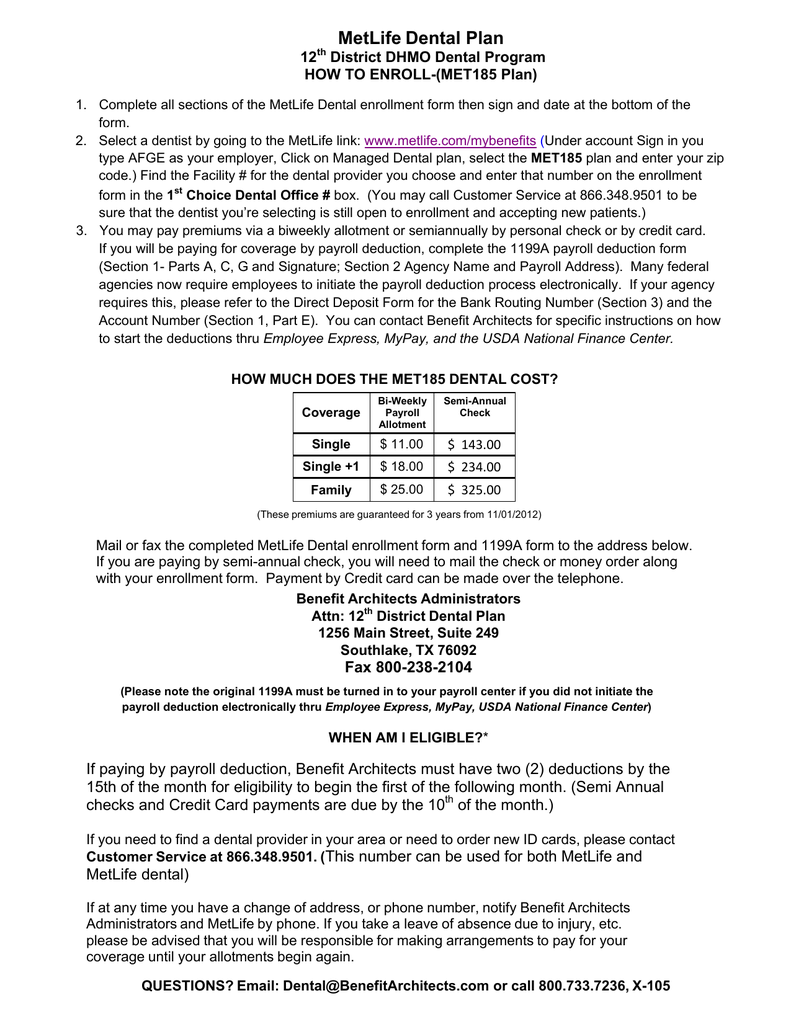
Metlife Dental Plan 12 Th District Dhmo Dental Program How To Enroll Met185 Plan Pdf Free Download
Metlife Dental Plan
