Nj Disability Temporary Insurance Form
Https Myleavebenefits Nj Gov Labor Myleavebenefits Assets Pdfs Pr 1 20 4 19 Ui Tdi Poster Pdf

Starbucks Job Application Form Pdf Job Hunter Database Employment Application Job Application Form Printable Job Applications
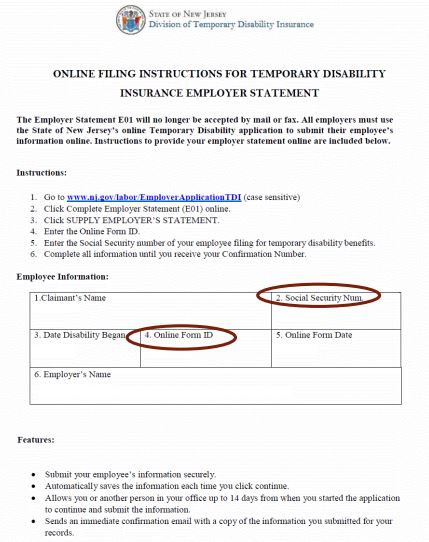
Division Of Temporary Disability And Family Leave Insurance How To Complete An Employer Statement
.jpg)
Division Of Temporary Disability And Family Leave Insurance Do You Need To Download A 1099 G
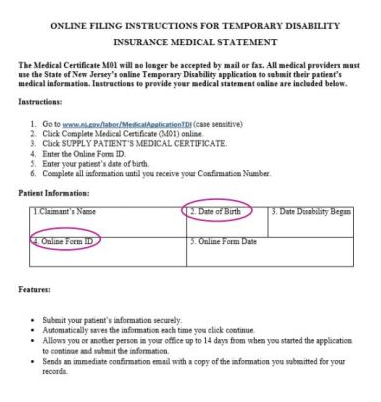
Division Of Temporary Disability And Family Leave Insurance How To Complete A Medical Statement
Fl2 Form Nj Fill Out And Sign Printable Pdf Template Signnow

New jersey s temporary disability and family leave insurance programs get more information check claim status or apply for benefits.
Nj disability temporary insurance form. This form is mailed only when your benefit payments are about to stop. Division of temporary disability insurance po box 387 trenton nj 08625 0387. If you still have more time left before your temporary disability insurance benefit payments are set to stop wait to receive this form in the mail before proceeding to our online service. It is intended for use by insurance companies employers union welfare funds and claims consultants who process and pay new jersey temporary disability claims under approved private plans.
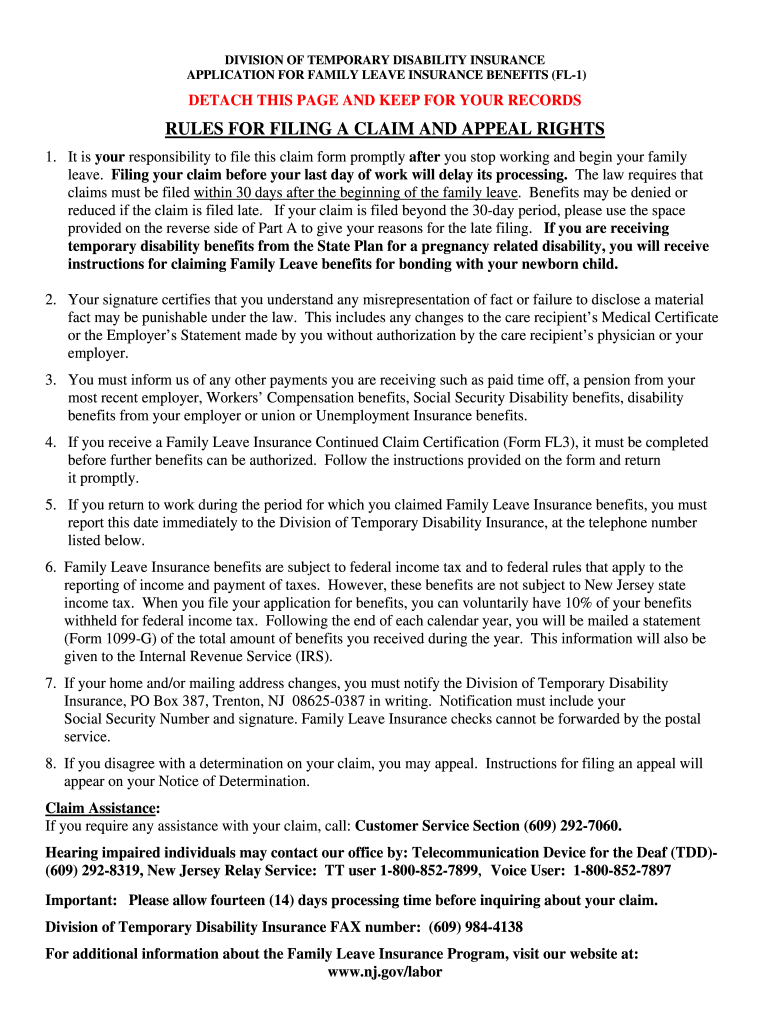
Temporary disability insurance application ds 1 download now family leave insurance application fl 1 download now. To secure a medical certification from the attending physician to support the claim part b. Official site of the state of new jersey. Print clearly and answer all questions or your benefits may be delayed.
After being approved for temporary disability benefits you may receive a form p 30 request to claimant for con tinued claim information use this form to claim additional benefits. Most employers in new jersey are required to have temporary disability insurance for their employees. Claim for disability benefits form ds 1. Welcome to the new jersey division of temporary disability insurance web application.
To notify the employer that the worker is claiming temporary disability benefits. Governor phil murphy lt. Temporary disability insurance provides cash benefits to new jersey workers who suffer an illness injury or other disability that prevents them from working and wasn t caused by their job. Printable application forms can be mailed to the address or faxed to the number on on each form.
This application allows physicians to file the documentation necessary to process their patient s new jersey state temporary disability benefits claim. New jersey temporary disability insurance application you are responsible for having your healthcare provider and employer complete parts b c of this application. This manual describes the benefits and eligibility conditions for approved private plans that are equal to the state plan in every way.

Fillable Online Lwd Dol State Nj New Jersey Temporary Disability Insurance Application Lwd Dol State Nj Fax Email Print Pdffiller
Https Www Abetterbalance Org Wp Content Uploads 2016 11 2015 Nj Family Leave Guide Pdf

Which Of These Windows Os Is Your Favorite Technology Tech Electronics Gadgets Instatech Device Gad Apple Iphone Latest Tech Geek Stuff

An Investment In Knowledge Always Pays The Best Interest Certifiedfinancialplanner Sip In 2020 Mutual Funds Investing Certified Financial Planner Financial Planning

Personal Disability Insurance Is The Most Reliable Form Of Protection For Your Paycheck In 2019 Learn More Disability Insurance What Is Disability Disability

Federal And State Labor Posters

Division Of Temporary Disability And Family Leave Insurance Information For Healthcare Providers
Division Of Temporary Disability And Family Leave Insurance Information For Employers
Https State Nj Us Health Medicalmarijuana Documents Id Cards Government 20assistance 20samples Pdf

Division Of Temporary Disability And Family Leave Insurance

Workers Compensation State By State Infographic Worker Compensation Car Insurance Comparison

Workers Compensation State By State Infographic Worker Compensation Car Insurance Comparison
Division Of Temporary Disability And Family Leave Insurance Why Did I Get This Form Look Up
