Refusal Workers Compensation Insurance Form

Vf 5001 General Verdict Form Single Plaintiff Single Defendant Multiple Causes Of Action Jury Instruction Form
Https Sbwc Georgia Gov Document Board Form Wc 10 Download

This Is A Connecticut Form That Can Be Used For Workers Compensation Connecticut Ms Word Compensation

Owners Damages For Breach Of Construction Contract Work Does Not Conform To Contract Construction Contract Instruction Jury
Https Www Wcrb Org Forms Xs Wc 0001 0002 Wi 10 14 Excess Workers Compensation And Employers Liability Coverage Pdf

Breach Of Implied Warranty Of Correctness Of Plans And Specifications Essential Factual Elements Instruction Jury Whistleblower

I hereby elect to reject workers compensation insurance coverage based on c r s.
Refusal workers compensation insurance form. Should i need medical attention at a later date i will notify my employer immediately. Tdi form number description file format language. By signing this form i realize that i do not necessarily affect my later eligibility for workers compensation. My signature below documents my refusal of medical attention and acknowledges that i was provided a dwc1 workers compensation claim form and notice of potential eligibility by my employer on the date noted.
A workers compensation policy must be current to reject coverage from. The form must be completed fully and accurately and must be signed by the officer rejecting coverage and by a representative of the employer. Court of workers compensation claims. Workers compensation insurance is required by law for all washington employers.
We assist injured workers employers health care providers and insurers in following the florida workers compensation rules and laws. Standard form medical report. I hereby acknowledge my refusal of medical treatment and or observation offered to me at the expense of renaissance staffing for the work related injury i incurred on. Our goal is to ensure that anyone interested or involved in the florida workers compensation system has the tools and resources they need to participate.
By signing this form you are acknowledging your rejection of all benefits under the workers compensation. Florida workers compensation uniform medical treatment status report form effective june 25 2006 rev. Petition for benefits determination settlement only. Select save target as to save the form in your personal files.
The business should be active in state corporation commission. 2430 chandler court sw po box 42401 olympia wa 98504 2401 360 753 6823 board of industrial insurance appeals. Workers compensation agreement forms. Florida workers compensation laws require employees to avail themselves of workers comp if they were injured on the job.
8 41 202 non agricultural. Court of workers compensation claims. Dwc081 agreement between general contractor and sub contractor to provide worker s compensation insurance rev. 1 31 2008 to access the interactive form right click the link.
Welcome to the division of workers compensation. Court of workers compensation claims.

Contractors Claim For Additional Compensation Abandonment Of Contract Jury Instruction Construction Contract
Workers Compensation Insurance Plan Acord Forms

Sufficiency And Service Of Notice Of Termination For Nuisance Or Unlawful Use Jury Instruction Ms Word

Workers Comp Affidavit Fill Online Printable Fillable Blank Pdffiller Pdffiller
Https Frg Wolterskluwer Com Workers Compensation Claims Pdf

Texas Workers Comp Exemption Form Fill Online Printable Fillable Blank Pdffiller
Workers Compensation Attorney Los Angeles Compensation Attorneys Worker
Http Dph Illinois Gov Sites Default Files Forms Workers Comp Opt Out 042616 Pdf
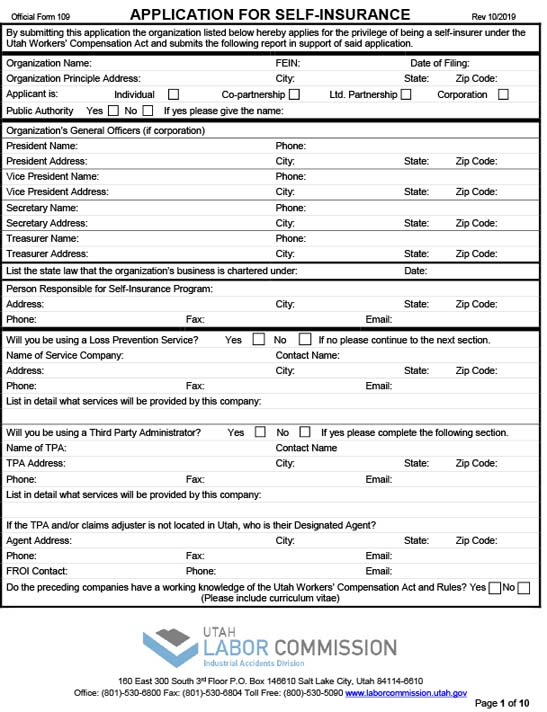
Industrial Forms Utah Labor Commission
Https Www Dol Gov Owcp Dfec Icstraining Filingforcompensationbenefits Filingforcompensationbenefits Pdf

Workers Compensation Attorney Los Angeles Compensation Worker Attorneys

Christopher J Smith P A Employee Earnings Reports Florida Workers Compensation

Workers Compensation Disability Approval Guide Workers Compensation Insurance Workplace Accident Worker