Self Insurance Form 1500

Amazon Com Tops Cms 1500 Health Insurance Claim Forms For Laser Printer 8 5 X 11 Inches 250 Sheets Per Pack 50135rv Office Products

What Are Superbills And Cms 1500 Forms Healthie

Amazon Com New Cms 1500 02 12 Claim Form 25 Forms Business Claim Forms Office Products

The Nutritionist S And Dietitian S Guide To Accepting Insurance
How To File For Insurance Reimbursement For Therapy Marsha Lucas Phd Psychologist
Https Www Dol Gov Owcp Dfec Regs Compliance Owcp 1500 Pdf

When a physician has a private practice but performs services at an institutional facility such as a hospital or outpatient facility the cms 1500 form would be used to bill for their services.
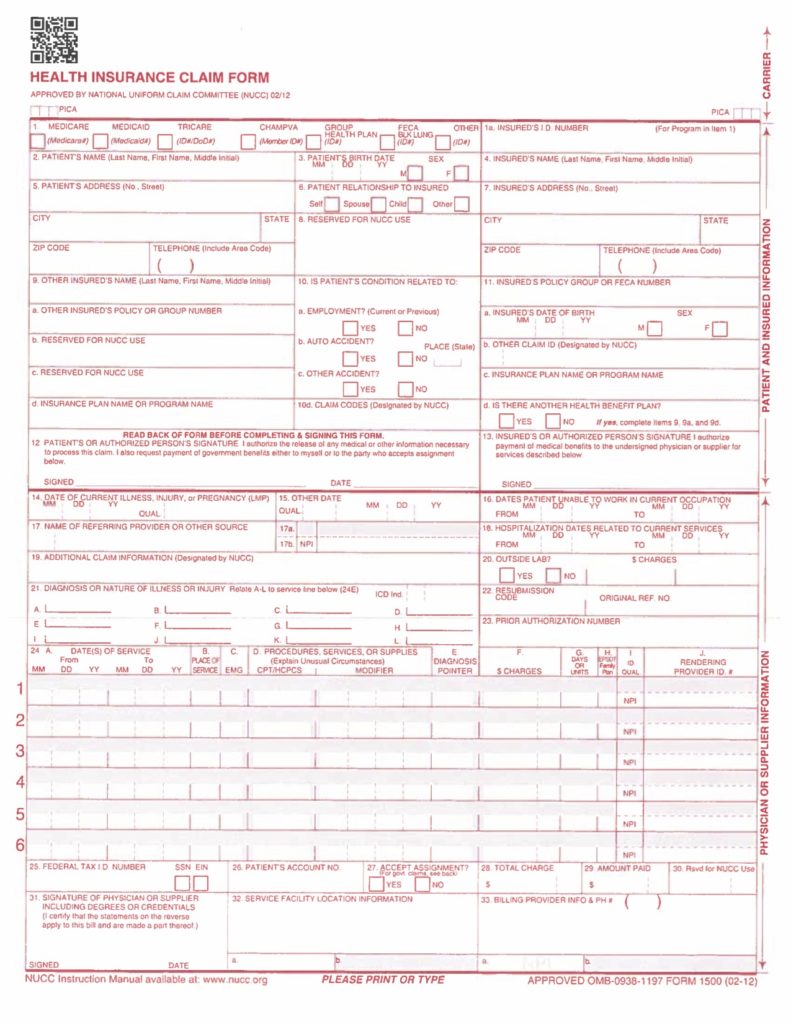
Self insurance form 1500. The cms 1500 form is the health insurance claim form used for submitting physician and professional claims for providers. Download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. In addition to medicare parts a b and for medicare durable medical equipment administrative contractors. 31 required signature of physician or supplier.
All items must be completed unless otherwise noted in these instructions. The cms 1500 form health insurance claim form is sometimes referred to as the ama american medical association form. The center of medicaid and medicare services cms form 1500 must be used to bill sfhp for medical services. Self insurance vocational reporting form f207 190 000 self insurance vocational services closing cover sheet f207 171 000 self insured employers medical only claim closure order and notice f207 020 111 f207 020 999.
Amount due after other insurance applied all contractual reductions. The signature can be printed stamped typed or hand signed but must be the name of a person not a facility. A cms 1500 with field descriptions and instructions is included in the link below. For a medicare crossover claim or medicare replacement plan claim leave this field blank.
The cms 1500 form is the standard paper claim form used by a non institutional provider or supplier to bill medicare carriers and medicare administrative contractors macs when a provider qualifies for a waiver from the administrative simplification compliance act asca requirement for electronic submission of claims. Approved omb 093b 1197 form cms 1500 06 15 omb no. Instructions for completing owcp 1500 health insurance claim form for medical services provided under the federal employees compensation act feca the black lung benefits act. A valid signature is required.
The cms 1500 form is the prescribed form for claims prepared and submitted by physicians or suppliers whether or not the claims are assigned. Self insured employers permanent partial disability closure order and notice ppd ntl f207 165 000. 1500 approved omb 0938 0999 form cms 1500 08 05 because this form is used by various government and private health programs see separate instructions issued by applicable programs. When you receive your explanation of medicare benefits papers attach copies to your hcfa 1500 claim forms.
Other insured s name last first middle initial.
Health Insurance Claim Form And Pip

New Cms 1500 Claim Forms 2500 Sheets 02 12 Version For Laser Or Inkjet Printers 1 Part Laser 2500 S Best Health Insurance Health Insurance Medical Claims
Https Files Medi Cal Ca Gov Pubsdoco Outreach Education Workbooks Modules Bb Cms1500 Bb Pdf
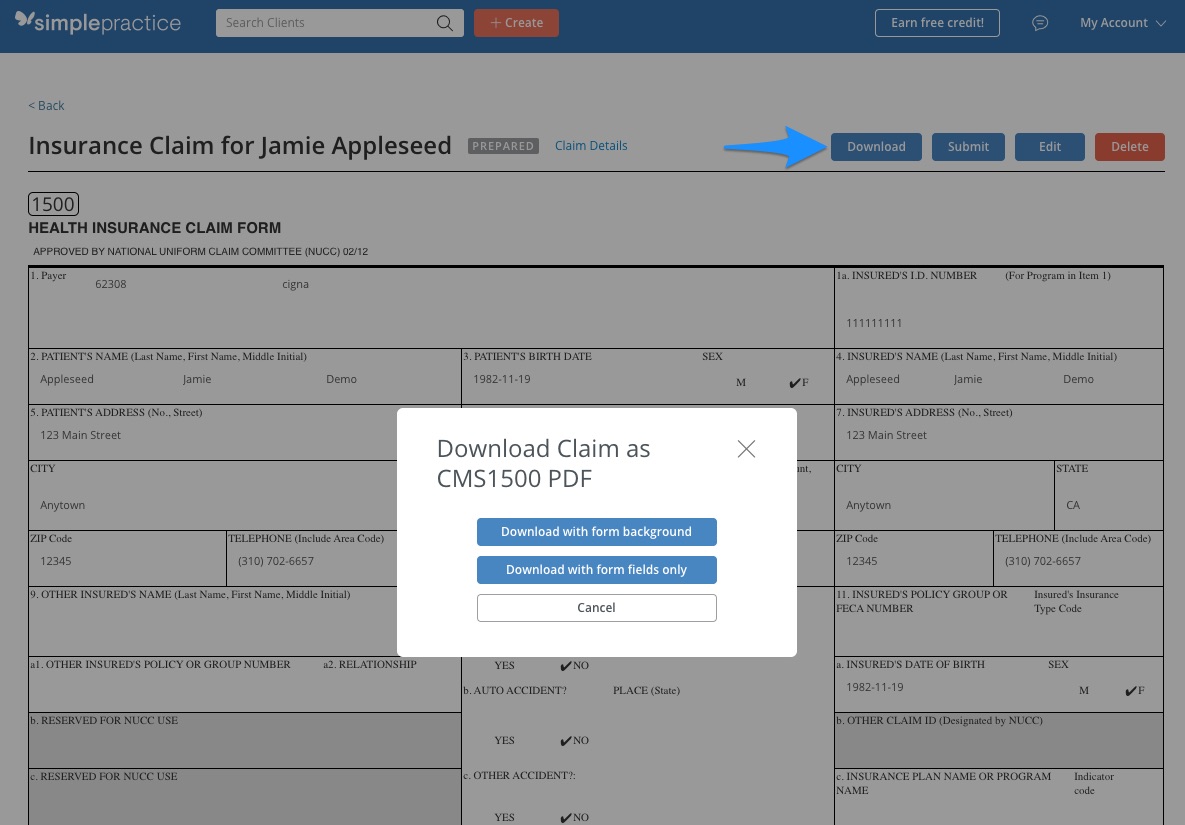
Creating And Printing A Cms 1500 Hcfa Claim Form Simplepractice Support

1500 Claim Form Template Health Insurance Claim Form Cms1500 Hosa In 2020 Health Insurance Free Health Insurance Business Letter Template

Cms 1500 Claim Forms And Other Medical Office Supplies Medical Claims Health Insurance Medical Insurance

Insurance Collect Eligible

Hcfa 1500 Cms 1500 Form Filler Software Allows You To Fill Out And Print Claim Forms A Simple Interfac Medical Claims Health Insurance Medical Insurance
Cms 1500 Health Insurance Paper Claim Forms 02 12 Free Priority Shipping Health Insurance Medical Claims Home Health Care
Https Www Oxhp Com Secure Materials Employer Lg Ba Guide 2008 Claims Pdf

Tops Centers For Medicare And Medicaid Services Forms 8 1 2 X 11 500 Forms Pack 50126rv Best Health Insurance Health Insurance Medical Claims
Http Manuals Medicaidalaska Com Docs Dnld Billing Cms1500 0212 Instructions Pdf

My New Blog Healthcare Efficiency Has Been Posted It Examines How Healthcare Claims Are Mishandled Www Howeverview Co Health Care Health Insurance Health
