Star Health Insurance Claim Form Part B

Most Up To Date Photo Star Health Claim Form 11 Stereotypes About Star Health Claim Form That Aren T Alwa Family Health Health Insurance Best Health Insurance

Star Health Claim Form Ten Features Of Star Health Claim Form That Make Everyone Love It Health Insurance Humor Free Dental Mother Health
Icici Lombard Health Insurance Claim Form Fill Online Printable Fillable Blank Pdffiller

Health Insurance Claim Medical And Health Reimbursement With Stethoscope On Cli Affiliate Clai Medical Health Insurance Health Insurance Dental Insurance

20 Car Insurance Certificate Template Dannybarrantes Temp In 2020 Certificate Of Achievement Template Certificate Of Participation Template Certificate Templates

Latest Pictures Hottest Totally Free Star Health Insurance Company Free Compare Plan Premium B Suggestions In 2020 Health Insurance Policies Health Insurance Health Insurance Companies
No 15 balaji complex whites lane 1st floor royapettah chennai 600 014.
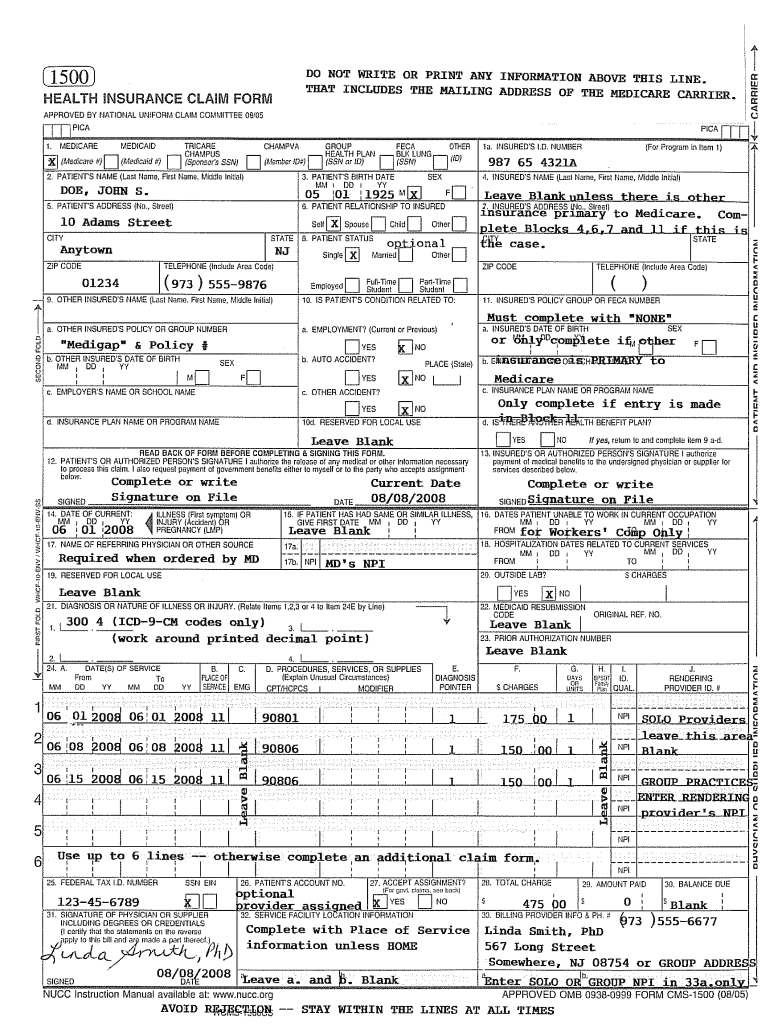
Star health insurance claim form part b. Star health and allied insurance co ltd with more than 400 offices and 8500 hospitals across india becomes the first private self contained indian insurance company. I new tank street valluvarkottam high road chennai 600 034. C name of the treating doctor. Star health and allied insurance claim form is divided into two parts part a which can be filled at home and part b which specifically has to be filled at the hospital as you may require guidance.
To be filled in by the hospital the issue of this form is not to be taken as an admission of liability please include the original preauthorization request form in lieu of part a. To be filled in block letters details of hospital a name of the hospital. Claims form download claims faqs. Claim form part b.
C name of the treating doctor. Corporate office claims dept. Claim form for medical insurance customer id issuance of this form does not amount to admission of liability under the policy. Corona rakshak policy star health and allied insurance co ltd.
Shahlip21067v012021 corona kavach policy star health and allied insurance co ltd. The company s headquarters has been set up in chennai tamil nadu india and it has been active since 2006. Star health and allied insurance company limited corporate office. Details of the patient admitted c type of hospital.
And its representatives who is my health insurer to seek any medical information records from you or from the medical. Star health and allied insurance company limited regd. If non network fill section e f registration no. No 15 1st 2nd floor sri balaji complex whites lane whites road royapettah chennai 600014.
Phone 044 2888 6495. To be filled in block letters a name of the hospital. Claim form part b to be filled in by the hospital the issue of this form is not to be taken as an admission of liability please include the original preauthorization request form in lieu of part a to be filled in block letters details of hospital a name of the hospital. Claim form part b.
To download the complete star health insurance claim form star health and allied insurance claim form click here. Toll free phone no. To be filled in by the hospital the issue of this form is not to be taken as an admission of liability please include the original preauthorization request form in lieu of part a. Shahlip21066v012021 star group covid insurance policy indemnity plan shahlgp21115v012021.
1800 425 2255 toll free fax no.

Remax Themed Transaction Management Form Real Estate Business Plan Real Estate Client Lead Generation Real Estate

Young Star Insurance Policy

Comprehensive Health Insurance Policy Starhealth In

Star Diabetes Safe Insurance Policy Star Health Insurance Health Insurance Best Health Insurance Insurance Policy
Star Health Insurance Coimbatore Family Health Optima Policy Premium

Original Medicare Medicare Advantage Plans At A Glance Medicalinsurancecoverage Medicare Advantage Medical Social Work Medicare

Process Of Finding Medicare Insurance Coverage Infographic Medicare Insurance Coverage Medicare Advantage

Best Medicare Videos Chris Westfall Youtube Medicare How To Plan Free Youtube

Star Health Insurance Online Quotes Renewal Reviews

Health Insurance Marketplace Form Health Insurance Plans Marketplace Health Insurance Private Health Insurance

Beware Of Scammers Using Medicare To Defraud You Medical Insurance Medicare Types Of Health Insurance
Star Health Insurance Agent Visiting Card Insurance

When You Turn 65 And Are Still Working You Have Several Options For Your Medical Insurance Coverage If You Have Creditable Coverage Through An Employer You H Home Health Care Home
