Tricare Third Party Libility Insurance Form

Dd Form 2527 Pdf Fill Online Printable Fillable Blank Pdffiller

2019 Form Dd 2527 Fill Online Printable Fillable Blank Pdffiller

Dd Form 2642 Tricare Dod Champus Medical Claim Defense
Dd Form 2642 Fill Out And Sign Printable Pdf Template Signnow
Https Tricare Mil Media Files Tricare Forms North Prime Enrollment N Ashx
Best Dd 2527 Us 2019 Update Formspro Io
Tricare east region attn.
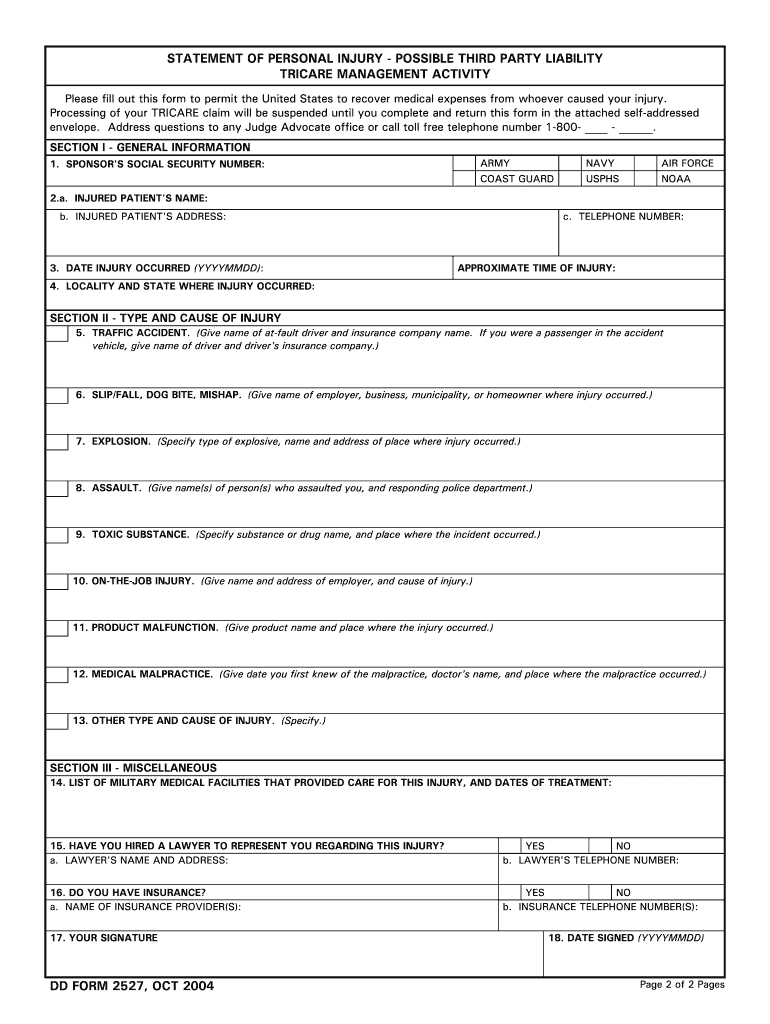
Tricare third party libility insurance form. If accident or work related the patient is required to complete dd form 2527 statement of personal injury possible third party liability. When tricare receives claims with these types of diagnosis codes we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. For all tricare dental program forms click here. For all active duty dental program forms click here.
Third party liability p o. Your regional contractor will send you the statement of personal injury possible third party liability dd form 2527 if a claim is received that appears to have third party liability involvement. Box 8968 madison wi 53707 8968 fax. Claims submitted with diagnosis codes 800 999 for professional services exceeding 500 and inpatient services often indicate an accidental injury or illness.
When filing these claims the provider needs to have the beneficiary complete the possible third party liability form. The grievance may be against any member of your health care team. Third party liability claim form. Request authorization for disclosure of health information.
This includes your tricare doctor your contractor or a subcontractor. Sometimes tricare receives claims that include diagnosis codes that may or may not relate to an injury. Describe condition for which patient received treatment supplies or medication. Public facility use certification form.
Dd2527 Fill Out And Sign Printable Pdf Template Signnow
Https Manuals Health Mil Displaymanualpdffile To08 98 Asof To08 C10s5 Pdf

How To Mail Dd Fill Online Printable Fillable Blank Pdffiller

2004 Form Dd 2527 Fill Online Printable Fillable Blank Pdffiller

Dd Form 2877 Tricare Prime Disenrollment Request Humana

Dd Form 2642 Download Fillable Pdf Or Fill Online Champus Claim Patient S Request For Medical Payment Templateroller
Free 8 Sample Tricare Authorization Forms In Pdf Ms Word

Third Party Liability Tricare
Https Www Specialneedsalliance Org Wp Content Uploads 2015 11 Elephants In The Room Pdf
Https Www Reginfo Gov Public Do Downloaddocument Objectid 59692200
Reconsideration Request Form Tricare Overseas
Dd Form 2876 3 Download Fillable Pdf Or Fill Online Tricare Prime Enrollment Disenrollment And Primary Care Manager Pcm Change Form Templateroller