Where Do I Mail Termination Of Insurance Form To Health First Insurance

Billing And Insurance Faqs

Student Health Insurance Requirement Health Network
Https Www Dol Gov Sites Default Files Ebsa About Ebsa Our Activities Resource Center Faqs Hipaa Compliance Pdf
Open Enrollment 2021 Guide Healthinsurance Org

Health Insurance Crossword Puzzle Wordmint

How To Handle Employees Who Want To Waive Health Insurance Coverage

You may also want to check the billing codes for medical errors and contact your health provider if you.
Where do i mail termination of insurance form to health first insurance. Frs health insurance subsidy certification for investment plan members. Option 1 you have group life insurance through work. A notice that is mailed is considered to be received 5 days after the date on the notice. Health insurance cancellation letter.
Zip code phone number. Centers for medicare medicaid services. The completion of this form is needed to document your voluntary request for termination of. It will eliminate any errors that may be made in the claim process and make it easier for you to re file your health insurance claim if it gets lost.
Individual insurance coverage termination form maryland washington d c and northern virginia not for coverage obtained through the federal exchange mail administrator. 410 505 2901 or toll free 800 305 1351. Frs investment plan termination and reemployment after receiving the health insurance subsidy benefit. Where your coverage comes from makes a difference when it comes to the forms you fill out.
Frs application for health insurance subsidy for investment plan members. Health insurance providers for example health insurance companies send this form to individuals they cover with information about who was covered and when. You are correct that the aca instituted a new 30 day notice requirement that applies toinsurers and plans if coverage will be rescinded. And to do that a formal health insurance cancellation letter has to be submitted to the insurance company.
Your full name street address. This letter to cancel an insurance policy has to be short and well framed one. Group life disability claims. Once you have your claim form filled out and your itemized bills from your doctor don t forget to make copies of everything.
The employee s employing office must either give the notice directly to the person eligible for tcc or send it by first class mail. You can complete and submit the group life claim form pdf. 05 21 request for termination of premium hospital and or supplementary medical insurance. You can use form 1095 b for information on whether you and your family members had health coverage that satisfies the individual shared responsibility provision.
Choose the option below that best describes your situation. My information is listed below. Request for cancellation of insurance policy. I have obtained a policy with another company and am sending you this written notice to request cancellation of my current insurance policy.
There are various reasons because of which a person plans to cancel the health insurance. Principal life insurance company attn. Box 14651 lexington ky 40512 fax. The aca added a provision about giving an employee 30 days notice for cancelation of health insurance.
Bring or mail your election form to. Form approved omb no.

How To Write An Appeal Letter To Your Health Insurance Provider

Is Health Insurance Mandatory

Florida Medicaid Eligibility Enrollment And Expansion Healthinsurance Org
Https Www Priorityhealth Com Medicare Media 1f1ae5ef70c3424d8c1fafcceeb1a604 Ashx

Health Insurance Claim Process Infographic Health Insurance Health Insurance Humor Health Insurance Companies
Employee Health Insurance Program User Manual Ppt Download

Iowa And The Aca S Medicaid Expansion Eligibility Enrollment And Benefits Healthinsurance Org

Faqs Washington Healthplanfinder
Best Life And Health Insurance Company
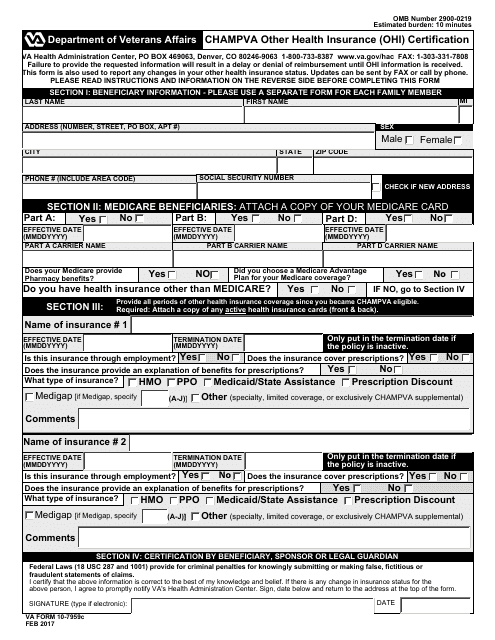
Va Form 10 7959c Download Fillable Pdf Or Fill Online Champva Other Health Insurance Ohi Certification Templateroller
Oscar Health Insurance Review Ny 2020 Safe Policies Insurance
