Workman Compensation Insurance Form 1010

1010 Form Fill Online Printable Fillable Blank Pdffiller Pdffiller
Form 1010 Download Fillable Pdf Or Fill Online Request Of Authorization Carrier Or Self Insured Employer Response Templateroller
Improper Use Of 1010 Form For Physician Referral
Https Frg Wolterskluwer Com Workers Compensation Claims Pdf
Http Www Dli Pa Gov Businesses Compensation Wc Claims Wcais Documents Wcais 20forms Libc 362 20int Pdf

Procedure Manual Feca Part 3 Division Of Federal Employees Compensation Dfec Office Of Workers Compensation Programs Owcp U S Department Of Labor
Suspension of prior authorization due to lack of information form 1010a is required to be filled out by carrier self insured employer and health care provider the requested treatment or testing is delayed due to a suspension of prior authorization due to lack of information to the carrier self insured employer on this the.
Workman compensation insurance form 1010. Case management and dispute resolution forms. Upon renewal of a workers compensation insurance policy a carrier may issue this label with updated policy information in lieu of issuing an entire new form c 105 poster as long as the current version of form c 105 is already being used. A list of contacts for questions regarding the filing or completion of the various claim forms can be found via this link contact information. Upon issuance of a certificate of election to be exempt the officer or member is not an employee and may not recover workers compensation benefits.
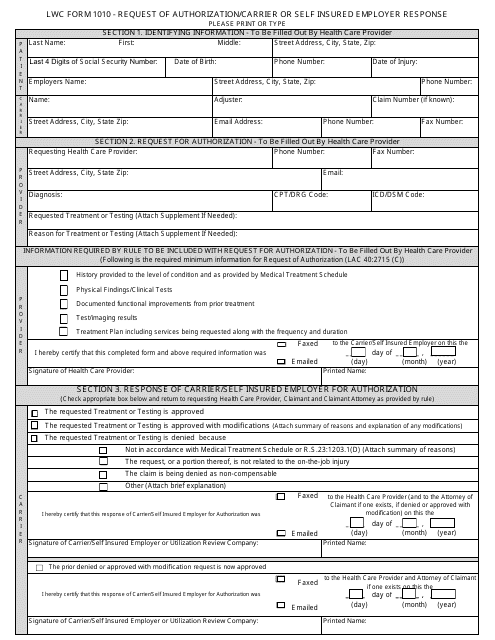
Lwc form 1010 request of authorization carrier or self insured employer response please print or type section 1. This label is placed over the expired policy information on the bottom of form c 105. Request of authorization carrier or self insured employer response form 1010. Lwc wc 1010 request of authorization carrier or self insured employer response.
The purpose of filing an exemption is for an officer of a corporation or member of a limited liability company to exclude themselves from the workers compensation laws. We assist injured workers employers health care providers and insurers in following the florida workers compensation rules and laws. The arkansas workers compensation commission s forms and other claims adjusting items are available for downloading or printing on the links below. The workers compensation training course for form 1010 and 1010a.
Welcome to the division of workers compensation. Unless otherwise noted the forms are provided in adobe pdf format. Identifying information to be filled out by health care provider first middle street address city state zip last name p a t i e n last 4 digits of social security number date of birth phone number employers name name adjuster c r email address date of injury claim number if known fax number section 2. The forms in the list below may be completed manually via the print form option or electronically via the electronic fill option.
Forms claims assistance. Many forms used in the workers compensation program are available from this page organized into the following categories.

Insurance
Http Www Katyisd Org Dept Hr Documents Nh 20para 20forms Pdf
Https Www Loudoun Gov Documentcenter View 153747 Workers Compensation Accident Report Packet

Insurance Carrier Contact Department Of Labor And Workforce

Getting Medical Care Approved In Louisiana Workers Compensation New Orleans Legal Llc

Ambulance Er Report Medpay Claim Auto Insurance Declarations Page Workman S Comp Claim Health Insurance Card Medpay Claim Pdf Free Download

Pa Workers Compensation Class Codes
Https Www Westmorelandinjurylawyers Com Pdf Libc 496 Pdf

Louisiana Workers Compensation Forms And Resources New Orleans Legal Llc
Louisiana Workers Compensation 101

2017 18 Non Tax Filer Student Kettering College

Your Rights Regarding Medical Records Authorization And Workers Compensation Claims

E4muksrx2t Snm